Injectable L-Carnitine: The Metabolic Shuttle Your Mitochondria Are Starving For
Your body makes about 20mg of L-Carnitine per day. You get another 100-300mg from food. And 95% of your total supply sits locked inside muscle tissue, doing one job: carrying fat into mitochondria so it can be burned for energy.
Without it, long-chain fatty acids pile up outside the mitochondrial membrane like delivery trucks stuck at a loading dock with no workers. The fuel is right there. The furnace is running. But nothing gets inside.
That is the carnitine shuttle. And it is the single most important bottleneck in human fat metabolism.
Oral L-Carnitine supplements line every GNC shelf in America. Most of them do almost nothing. Bioavailability sits between 14-20%. The rest gets destroyed in your gut, and worse, gut bacteria convert a significant portion into trimethylamine (TMA), which the liver oxidizes into TMAO, a metabolite linked to cardiovascular risk.
Injectable L-Carnitine changes the entire equation. 100% bioavailability. Zero gut bacterial conversion. Zero TMAO production. Direct delivery to circulation and target tissues.
This is why practitioners who understand pharmacokinetics stopped recommending oral L-Carnitine years ago. The injectable form is not just a better delivery method. It is a fundamentally different intervention.
KEY FACTS
Definition: L-Carnitine is a conditionally essential amino acid derivative that transports long-chain fatty acids into mitochondria for energy production
Primary Use: Fat metabolism optimization, athletic performance, androgen receptor upregulation, fertility support, cardiac health
Administration: Subcutaneous or intramuscular injection; 100mcg to 5g depending on application
Typical Timeline: Tissue saturation begins at 2-3 weeks; full metabolic adaptation at 8-12 weeks
Best For: Athletes seeking body recomposition, individuals with metabolic inflexibility, fertility support, cardiac health optimization
Not For: Those expecting a fat burner that replaces proper nutrition and training
What Is L-Carnitine?
L-Carnitine (beta-hydroxy-gamma-N-trimethylaminobutyric acid) is synthesized endogenously from the amino acids lysine and methionine. The process requires vitamin C, vitamin B6, niacin, and iron as cofactors. Synthesis occurs primarily in the liver and kidneys, with the final product distributed throughout the body.
The distribution is telling. Roughly 95% of total body carnitine resides in skeletal and cardiac muscle. The remaining 5% circulates in plasma, liver, kidneys, and brain. This extreme tissue concentration reflects how deeply embedded carnitine is in muscular energy production.
Your body exists in two main fuel states: glucose burning and fat burning. Carnitine is the gatekeeper that determines how efficiently you switch between them. This concept, called metabolic flexibility, underpins everything from athletic endurance to insulin sensitivity to body composition.
Several forms of carnitine exist in research and supplementation:
L-Carnitine is the base form and the most studied for injectable protocols. Acetyl-L-Carnitine (ALCAR) crosses the blood-brain barrier and targets cognitive function. Propionyl-L-Carnitine (PLC) concentrates in cardiac and vascular tissue. L-Carnitine L-Tartrate (LCLT) shows the strongest data for androgen receptor upregulation. Each serves a different biological niche, but injectable L-Carnitine provides the broadest systemic coverage.
The Science: How L-Carnitine Actually Works
The Carnitine Shuttle System
Long-chain fatty acids (C14 and longer) cannot cross the inner mitochondrial membrane on their own. Medium and short-chain fatty acids can diffuse passively, but the long-chain fats that make up the majority of stored body fat require active transport.
The carnitine shuttle operates in four steps.
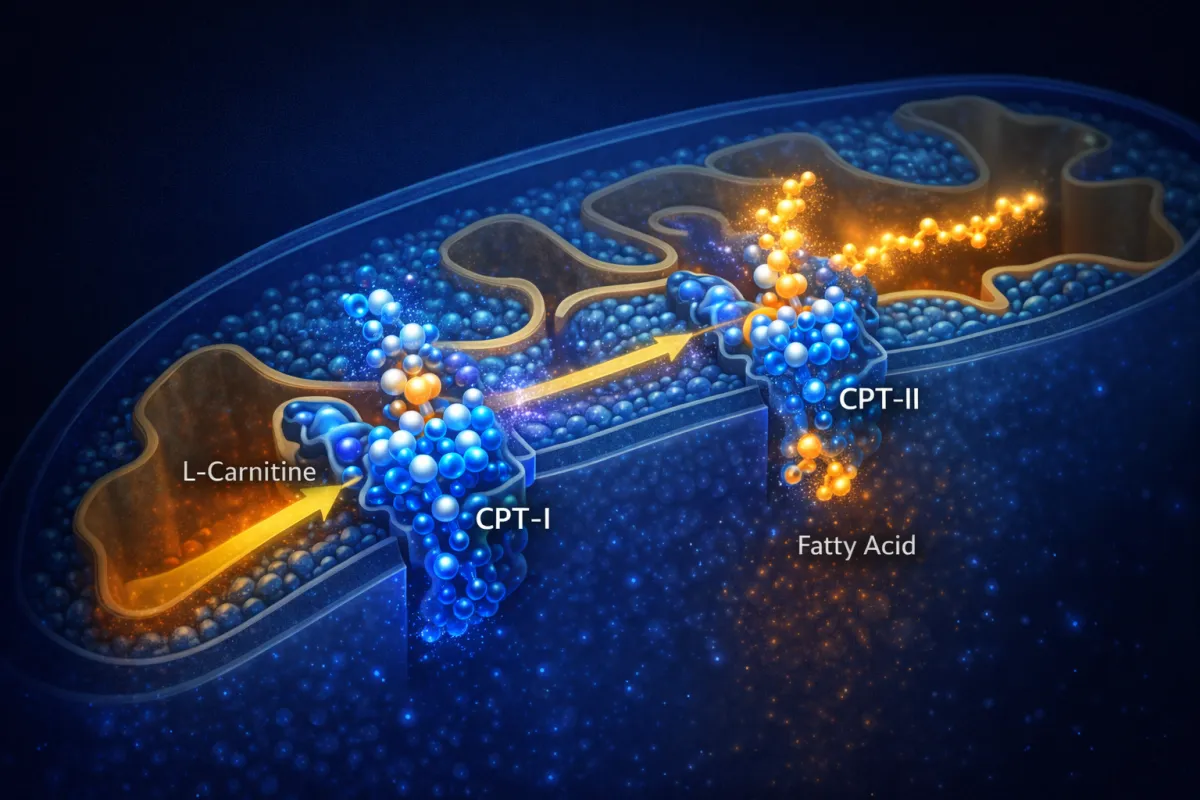
First, long-chain fatty acids are activated to fatty acyl-CoA by acyl-CoA synthetase on the outer mitochondrial membrane. Second, Carnitine Palmitoyltransferase I (CPT-I) transfers the acyl group from CoA to carnitine, creating acyl-carnitine. CPT-I is the rate-limiting enzyme in this entire process. Its activity determines your ceiling for fatty acid oxidation. Third, Carnitine-Acylcarnitine Translocase (CACT) shuttles acyl-carnitine across the inner membrane while simultaneously returning free carnitine to the intermembrane space. Fourth, Carnitine Palmitoyltransferase II (CPT-II) transfers the acyl group back to CoA inside the mitochondrial matrix, releasing free carnitine to repeat the cycle. The fatty acyl-CoA then enters beta-oxidation.
Think of it like a ferry system. The fatty acid is the passenger. Carnitine is the ferry. CPT-I loads passengers at the dock. CACT runs the ferry across the channel. CPT-II unloads passengers on the other side. More ferries mean more passengers crossing per hour. Saturating muscle tissue with carnitine increases the fleet size.
Acetyl-CoA Buffering
During high-intensity exercise, glycolysis produces pyruvate faster than mitochondria can process it through the Krebs cycle. Acetyl-CoA accumulates in the mitochondrial matrix, inhibiting pyruvate dehydrogenase (PDH) and forcing the cell toward anaerobic metabolism. Lactate builds. Performance drops.
L-Carnitine provides a pressure release valve. Carnitine Acetyltransferase (CAT) converts excess acetyl-CoA plus free carnitine into acetyl-carnitine plus free CoA. This clears the bottleneck, keeps the Krebs cycle running, and delays lactate accumulation. Research shows this mechanism extends time to exhaustion at threshold intensities between 70-85% VO2 max.
Androgen Receptor Upregulation
This is the mechanism most people miss entirely, and it may be the most significant for body composition.
Research from the University of Connecticut demonstrated that three weeks of L-Carnitine L-Tartrate supplementation at 2g per day significantly increased resting androgen receptor content in muscle tissue. Androgen receptors are the docking stations where testosterone binds to initiate muscle protein synthesis, recovery, and growth signaling. More receptors mean more binding sites. More binding sites mean your existing testosterone works harder.
The mechanism appears linked to carnitine's effect on cellular energy status. Enhanced mitochondrial function shifts the energy environment inside muscle cells, signaling the cell to upregulate androgen receptors. This effect was further amplified when subjects consumed protein and carbohydrates after resistance exercise.
Clinical experience shows this makes L-Carnitine particularly valuable for three populations: natural athletes maximizing endogenous hormone function, men on testosterone replacement therapy seeking greater receptor sensitivity, and aging individuals experiencing declining androgen receptor density.
CLINICAL TAKEAWAY: L-Carnitine does not increase testosterone levels. It increases the number and sensitivity of receptors that testosterone acts on, making your existing hormones more effective.
IGF-1 and mTOR Signaling
Improved cellular energy status from enhanced carnitine availability reduces chronic AMPK activation and shifts the balance toward mTOR signaling. This promotes protein synthesis and cellular growth. L-Carnitine may also enhance IGF-1 receptor sensitivity on muscle cells, creating a dual anabolic signal: better androgen receptor function plus enhanced growth factor signaling.
Fertility Mechanisms
In males, sperm cells are extraordinarily dependent on mitochondrial energy production. Flagellar movement requires massive ATP output. L-Carnitine enhances mitochondrial function in sperm, improving motility, reducing DNA fragmentation, supporting better morphology through improved acrosome formation, and protecting sperm mitochondria from oxidative damage. Meta-analyses of male infertility trials consistently show improvements across all sperm parameters with L-Carnitine supplementation.
In females, oocyte quality depends heavily on mitochondrial function. L-Carnitine supports meiotic spindle formation for proper chromosome segregation, enhances granulosa cell metabolism, improves response to FSH stimulation, and reduces oxidative stress in developing eggs. Research in women with PCOS has shown improved ovulation rates and higher pregnancy rates when L-Carnitine is combined with standard fertility treatment.
Cardiac-Specific Mechanisms
The heart derives 60-70% of its ATP from fatty acid oxidation, making it the most carnitine-dependent organ by metabolic demand.
Practitioners report a specific low-dose nocturnal protocol targeting cardiac iron chelation. At doses between 50-100mcg administered before bed, L-Carnitine chelates iron deposits in cardiac tissue during the energy-depleted nocturnal state. Iron-catalyzed free radical production is a primary driver of cardiac fibrosis and arrhythmia. This mechanism requires low dosing to avoid saturating general metabolic pathways and nocturnal timing to prioritize chelation during cellular rest.
Additionally, during ischemic events, toxic acyl-CoA accumulates in cardiac tissue. L-Carnitine converts these compounds to harmless acyl-carnitines, reducing infarct size. Post-myocardial infarction studies show L-Carnitine administration within 24 hours improves left ventricular function and reduces mortality at 12-month follow-up.
Research Evidence
Body Composition
A comprehensive meta-analysis of 37 randomized controlled trials (2,292 participants) found that L-Carnitine supplementation significantly reduced body weight by 1.21kg, BMI by 0.24 kg/m2, and fat mass by 2.08kg compared to placebo. Effects were most pronounced in overweight and obese subjects.
A 2025 umbrella meta-analysis published in the International Journal of Vitamin and Nutrition Research confirmed these findings across multiple pooled analyses, noting that effects followed a non-linear dose-response pattern for both weight and BMI changes.
The critical caveat: these meta-analyses primarily used oral supplementation. Injectable protocols achieving 100% bioavailability would be expected to produce more consistent and potentially larger effects, though direct head-to-head injectable meta-analyses remain limited.
Athletic Performance
A systematic review and meta-analysis published in PMC examining L-Carnitine supplementation in healthy subjects found significant improvements in VO2 at rest and significant increases in serum free and total carnitine at rest and after exercise. The optimal supplementation protocol for measurable carnitine level changes was 2g daily for 3-4 weeks.
The landmark Wall et al. study demonstrated that chronic L-Carnitine supplementation combined with carbohydrate co-ingestion successfully elevated muscle carnitine content, a finding previously thought impossible. This established the insulin-dependent OCTN2 transporter mechanism for driving circulating carnitine into muscle tissue.
Androgen Receptor Studies
Kraemer et al. (2006) at the University of Connecticut showed that 21 days of LCLT supplementation at 2g daily significantly upregulated pre-exercise androgen receptor content compared to placebo. Post-exercise feeding with protein and carbohydrates further amplified this effect, with the combination of LCLT plus post-workout nutrition producing the highest androgen receptor density.
Injectable vs. Oral Administration
A study examining hemodialysis patients switching from oral (900mg/day) to intravenous (1000mg) L-Carnitine demonstrated that IV administration significantly increased total, free, and acyl carnitine levels, decreased serum free fatty acids, and increased HDL-cholesterol within 1-4 weeks. This confirms the pharmacokinetic superiority of parenteral administration.
Cardiovascular Outcomes
The CEDIM trial (L-Carnitine Ecocardiografia Digitalizzata Infarto Miocardico) demonstrated that L-Carnitine administration post-myocardial infarction reduced infarct size, improved left ventricular remodeling, and decreased mortality at 12-month follow-up.
Aging and Cognition
A controlled clinical trial in centenarians showed L-Carnitine treatment reduced severity of both physical and mental fatigue while increasing cognitive functions. This is significant because it demonstrates benefits even in the most advanced aging population with the most depleted endogenous carnitine reserves.
Practical Protocols
Injectable L-Carnitine protocols span a wider dosing range than most compounds because different doses activate distinct biological mechanisms. The following tiers reflect clinical experience across multiple applications.
Tier 1: Cardiac Health (50-100mcg)
This protocol targets myocardial iron chelation and cardiac tissue protection.
PROTOCOL SUMMARY (TEXT): Typical dosing ranges from 50 to 100mcg subcutaneously before bed, administered daily for a minimum of 12-16 weeks. Nocturnal timing is essential because the energy-depleted cellular state during sleep allows chelation pathways to take priority over general metabolic functions.
Expected outcomes include gradual reduction in cardiac iron deposits, improved left ventricular function, reduced arrhythmia burden, and enhanced exercise tolerance. This tier suits post-MI recovery under medical supervision, heart failure management as adjunct therapy, and preventive cardiac health optimization.
Tier 2: Health Optimization (100-250mcg)
This tier targets general metabolic health, longevity support, and insulin sensitivity.
PROTOCOL SUMMARY (TEXT): Typical dosing ranges from 150 to 200mcg subcutaneously upon waking, administered daily on an ongoing basis. This represents the threshold dose for systemic metabolic effects without aggressive performance or body composition goals.
Expected outcomes include improved subjective energy, better metabolic flexibility, fasting glucose and triglyceride reductions, and fertility marker improvements. Ideal for health-conscious individuals targeting longevity, those with mild metabolic dysfunction, couples attempting conception, and aging individuals over 40 focused on mitochondrial health.
Tier 3: Athletic Performance (250mcg-1g)
Endurance athletes typically use 300-500mcg subcutaneously 30-60 minutes before training, with 200mcg on rest days. Strength and power athletes may use 500mcg to 1g intramuscularly 45-60 minutes before training, with 250-500mcg subcutaneously on rest days. Duration should cover a minimum 12-week mesocycle.
PROTOCOL SUMMARY (TEXT): Typical dosing ranges from 250mcg to 1g depending on training demands, administered subcutaneously or intramuscularly on training days and subcutaneously on rest days. Duration is a minimum 12-week block to allow full muscle tissue carnitine saturation.
Carbohydrate co-ingestion strategy is critical at this tier: consume 40-80g of fast-acting carbohydrates within 15 minutes of injection. The resulting insulin spike drives L-Carnitine into muscle tissue via OCTN2 transporters. Without this step, circulating carnitine clears renally before tissue uptake occurs.
Expected outcomes include improved fat oxidation at submaximal intensities, extended time to exhaustion, reduced lactate at threshold, and faster between-session recovery.
Tier 4: Body Recomposition (1-5g)
This is the maximum fat oxidation protocol for aggressive body composition changes.
PROTOCOL SUMMARY (TEXT): Typical dosing ranges from 2 to 5g daily for males and 1 to 2.5g for females, administered intramuscularly for volumes exceeding 1mL. Doses above 2.5g should be split between morning and pre-training. Carbohydrate co-ingestion of 40-80g post-injection is required. Duration is 12-16 weeks.
Expected outcomes include 0.5-1% body fat reduction per week when combined with a proper caloric deficit, muscle preservation during dieting, and maintained training intensity despite caloric restriction. L-Carnitine amplifies proper nutrition and training. It does not replace them.
Tier 5: Fertility Enhancement
Male protocol: 200-500mcg subcutaneously daily for a minimum of 90 days (one full spermatogenesis cycle). Female protocol: 100-250mcg subcutaneously daily, beginning 60-90 days before conception attempts. Both protocols should be discussed with a fertility specialist.
Gender-Specific Dosing
Clinical experience shows females generally respond to approximately 50% of male dosing across all tiers. This reflects differences in muscle mass distribution, hormonal milieu, and baseline carnitine metabolism. Starting conservatively and titrating based on response is standard practice.
What to Expect: Timeline
Week 1-2: Subtle energy improvements. Reduced post-exercise fatigue. Possible mild injection site warmth. Circulating carnitine levels rise but muscle tissue saturation has not yet occurred. Do not expect visible body composition changes.
Week 3-4: Measurable increase in androgen receptor density based on research data. Improved workout endurance becomes noticeable, particularly at threshold intensities. Metabolic flexibility begins improving. Fasting becomes easier. Carbohydrate tolerance improves.
Week 5-8: Muscle tissue carnitine saturation approaches optimal levels. Fat oxidation rates during exercise measurably increase. Recovery between sessions improves noticeably. Body composition changes become visible if nutrition and training are dialed in.
Week 9-12: Full metabolic adaptation. Peak androgen receptor density. Maximum fat oxidation capacity achieved. Athletic performance improvements plateau. Lab markers (fasting glucose, triglycerides, HDL) show meaningful shifts. This is the assessment point for whether to continue, adjust dosing, or cycle off.
Advanced Stacking Strategies
Stack 1: The Mitochondrial Powerhouse (L-Carnitine + SS-31)
L-Carnitine optimizes fatty acid transport into mitochondria. SS-31 (Elamipretide) stabilizes cardiolipin on the inner mitochondrial membrane, improving electron transport chain efficiency and reducing proton leak. Together, they address both fuel delivery and furnace efficiency. Add MOTS-C for mitochondrial-derived signaling peptide support and you have the most comprehensive mitochondrial optimization protocol available.
Protocol: L-Carnitine 500mcg daily + SS-31 per standard dosing + MOTS-C 10mg 2-3x weekly.
Stack 2: The Recomposition Engine (L-Carnitine + 5-Amino-1MQ)
L-Carnitine drives fat into mitochondria for oxidation. 5-Amino-1MQ inhibits NNMT (nicotinamide N-methyltransferase), increasing NAD+ availability and enhancing metabolic rate. The combination attacks body fat from two angles: increased transport to oxidation sites and increased basal metabolic activity.
Protocol: L-Carnitine 2-5g daily + 5-Amino-1MQ per standard dosing. Stack during caloric deficit phases for maximum effect.
Stack 3: The Anabolic Recovery Stack (L-Carnitine + BPC-157 + TB-500)
L-Carnitine enhances androgen receptor density and recovery capacity. BPC-157 accelerates tissue repair through growth factor upregulation. TB-500 reduces systemic inflammation and promotes cellular migration to injury sites. This combination optimizes the training-recovery-adaptation cycle for athletes in heavy training blocks.
Protocol: L-Carnitine 500mcg-1g pre-training + BPC-157 250-500mcg daily + TB-500 2-2.5mg 2x weekly.
Stack 4: The Fertility Protocol (L-Carnitine + CoQ10)
L-Carnitine supports mitochondrial energy production in reproductive cells. CoQ10 serves as a critical electron carrier in the mitochondrial electron transport chain and provides antioxidant protection. For males, this combination addresses motility, morphology, and DNA fragmentation simultaneously. For females, it supports oocyte energy reserves and meiotic integrity.
Protocol: L-Carnitine 200-500mcg daily + CoQ10 200-400mg orally. Minimum 90 days before assessment for males.
Stack 5: The Longevity Protocol (L-Carnitine + NAD+ + Epithalon)
L-Carnitine maintains metabolic flexibility as endogenous production declines with age. NAD+ restores sirtuin pathway activity for cellular repair and DNA maintenance. Epithalon activates telomerase for telomere length preservation. This stack addresses three of the primary hallmarks of aging: metabolic decline, NAD+ depletion, and telomere shortening.
Protocol: L-Carnitine 150-250mcg daily + NAD+ per standard dosing + Epithalon in standard cycling protocol.
Safety and Side Effects
Common Side Effects
Injection site reactions including mild warmth, redness, or transient stinging are the most frequently reported effects. These typically resolve within minutes. Body odor changes can occur at higher doses (particularly above 2g daily) due to trimethylamine excretion through sweat. Mild gastrointestinal discomfort is possible but far less common with injectable than oral administration. Nausea is rare.
The TMAO Question
This is the most important safety consideration with L-Carnitine, and it is also the strongest argument for injectable over oral administration.
Oral L-Carnitine is metabolized by gut bacteria into trimethylamine (TMA), which the liver converts to trimethylamine N-oxide (TMAO). Elevated TMAO is associated with increased atherosclerosis, cardiovascular events, and stroke risk. A 2024 review in Nutrients confirmed that gut microbial metabolism of L-Carnitine into TMAO remains a legitimate cardiovascular concern. A 2025 review in Exploration of Cardiology specifically compared short-term versus long-term oral L-Carnitine intake and concluded that chronic oral supplementation raises TMAO to clinically concerning levels.
Injectable L-Carnitine bypasses the gastrointestinal tract entirely. No gut bacterial exposure. No TMA production. No TMAO elevation. This is not a minor advantage. It eliminates the primary safety concern associated with L-Carnitine supplementation.
Research in 2024 identified the gbu gene cluster as the key microbial genes responsible for converting dietary L-Carnitine to TMA, with vegetarians showing more dramatic increases in TMAO-producing bacteria after oral carnitine exposure than omnivores. This confirms the gut microbiome-dependent nature of TMAO production and further validates injectable administration as the pharmacokinetically superior route.
Contraindications
Individuals with seizure disorders should exercise extreme caution. The FDA prescribing information for injectable levocarnitine notes that increased seizure frequency and severity have been reported in patients with pre-existing seizure activity.
Those with severe kidney disease should consult their physician before use, as TMAO clearance depends on renal function and carnitine metabolism may be altered in kidney disease.
Hypothyroidism may be aggravated by L-Carnitine. Research suggests carnitine inhibits thyroid hormone entry into cell nuclei. Individuals with thyroid conditions should monitor thyroid panels during use.
Drug Interactions
Anticoagulants (warfarin): L-Carnitine may potentiate anticoagulant effects. Monitor INR if combining. Thyroid medications: Potential interference with thyroid hormone cellular uptake. AZT (zidovudine) and valproic acid: Both drugs can reduce carnitine levels; supplementation may be beneficial but should be medically supervised.
Monitoring Recommendations
Baseline and quarterly metabolic panels are prudent for long-term use. Lipid panels every six months. Thyroid panels if symptoms warrant. Subjective tracking of energy, recovery, and exercise tolerance provides the most immediate feedback.
Trusted Sources
Quality matters with injectable compounds. Third-party testing and proper handling make the difference between a product that works and one that introduces contaminants directly into your body.
Vetted suppliers with Certificates of Analysis:
Optimum Formula - Code: BHACK (10% off) - L-Carnitine 1000mg injectable
LimitlessBioChem EU - Code: BHACK (10% off) - L-Carnitine Solution 500mg/ml
BioLongevity Labs - Code: BHACK (15% off) - L-Carnitine injectable
For complete vendor comparison: biohackblueprint.io
Additional vetted research suppliers:
Modern Aminos - Code: zach10 (10% off)
ResearchChemHQ - Code: BHACK
BioSLab Canada - Code: BHACK (10% off)
Limitless Life Nootropics - Code: BHACK (15% off)
Always verify Certificates of Analysis and third-party testing before purchasing any injectable compound. Look for HPLC purity testing above 98%, sterility testing documentation, and proper cold chain shipping.
The Bigger Picture
L-Carnitine is not glamorous. It does not have the mystique of growth hormone secretagogues or the healing reputation of BPC-157. It is a metabolic workhorse that has been overshadowed by decades of ineffective oral supplement marketing.
The injectable form corrects the fundamental limitation that made oral L-Carnitine disappointing. When you bypass the gut, you bypass the bioavailability problem and the TMAO risk simultaneously. What remains is one of the most well-researched, broadly beneficial compounds available: fat metabolism optimization, androgen receptor upregulation, fertility support, cardiac protection, and mitochondrial enhancement from a single molecule.
The dosing spectrum is unusually wide because carnitine operates across multiple biological systems. A 50mcg nocturnal dose for cardiac iron chelation and a 5g pre-training dose for maximum fat oxidation are not the same intervention, even though they use the same molecule. Understanding which tier matches your goals is essential.
For most people starting out, Tier 2 (100-250mcg daily) provides the broadest benefit with the simplest protocol. Athletes and those pursuing active body recomposition can scale to Tier 3 or 4 with appropriate nutritional support. The carbohydrate co-ingestion strategy is not optional at higher doses. Without the insulin-mediated OCTN2 transporter activation, most of your injected carnitine clears through the kidneys before reaching muscle tissue.
Final Thoughts
L-Carnitine represents a rare category in the research compound space: a molecule where the science is robust, the safety profile is well-established, the mechanisms are clearly understood, and the primary historical limitation (oral bioavailability) has a clean solution.
If you are already optimizing your mitochondrial health, training seriously, or pursuing fertility goals, injectable L-Carnitine fills a metabolic gap that few other compounds address. If you are looking for a standalone fat burner to compensate for poor dietary habits, look elsewhere. Carnitine amplifies good fundamentals. It does not replace them.
The androgen receptor upregulation data alone makes this compound worth investigating for any male interested in maximizing hormonal efficiency without exogenous hormone use.
What is your experience with L-Carnitine? Are you using oral or injectable? Have you noticed differences between forms? Drop your protocol and timeline below.
Disclaimer: This content is for educational and research purposes only. Peptides are not approved for human use. Nothing here is medical advice. Consult a qualified professional for personalized guidance.
